Health officials need to learn to quit issuing well-intended but conflicting advice to the public. Especially, when coronavirus infections spike or when the officials start restricting citizens.
Our government took excellent action in January by quickly placing constraints on entry into U.S. airports by travelers arriving from countries infected with the Wuhan, China coronavirus. And behind the scenes there may be other excellent actions. However, since the sudden cluster of coronavirus victims and deaths in Kirkland, Washington officials on the federal government’s containment-team, as well as esteemed doctors from around the country, have been communicating well-intended but conflicting advice to the public. How poor? Much of the public ignored it. And the city of Kent, Washington sued its county health officials.
Why am I speaking up when I’m no doctor? First, we all have skin in this game. In my case, my grandparents lived in Kirkland Washington for 50+ years, while much of my remaining family resides in the Seattle-Tacoma-Everett area.
Second, we need to rapidly surface and share the best containment and self-protection techniques during this pandemic. Not just locally — but city to city and nationally. Additionally, my background in high performing systems behavior caused me to spot some early mistakes and ineffective communications by federal, state, and city teams trying to do their best during the first fast-spiking virus-cluster in the U.S.
I comment based upon the following perspective:
>> High performing systems (HPS) learn faster than their opponent.
>> High performing systems have a quick feedback loop that identifies what’s working & not working well, and shares this information across the team, seeking a fix. (If the latest new-hire on the team has a better fix than the president of the company — fine!)
>> Low performing systems bicker and blame instead of focusing on fixes.
Therefore, the following assessment is intended to set aside personal blame and instead encourage people on the front-lines of the pandemic to routinely use HPS techniques.
High performance teams communicate clearer than lower performing teams.
While I was recently in Seattle, the Seattle KOMO TV report of February 26. excellently captured the similarity of advice from multiple expert sources about how people should self-protect. Below, in brown text, is a summary of that advice from federal containment personnel, along with national and local TV / radio talk-show doctors. The advice commonly includes the phrases “average person” or “general population”. Those phrases mean people in normal low-risk daily influenza conditions.
>> CDC doesn’t recommend people use face masks.
>> Only wear a face mask if you are sick.
>> Don’t buy and don’t wear face masks for protection against the coronavirus.
>> We don’t have enough masks for U.S. caregivers.
>> Better to lower the risk to caregivers than lower the risk for the general public.
>> Don’t panic.
But what wasn’t said by the experts?
There was no advice on what happens if low-risk conditions in your neighborhood or workplace swiftly turn into high-risk conditions. And that’s exactly what surfaced on February 29th at the Life Care Center of Kirkland, Washington, along with the subsequent movement of infected people into the EvergreenHealth Medical Center.

After the outbreak and as the death count rose, federal, state, or city officials who were leading the pandemic-containment effort did not tell the public that there was a significant change in risk status within one facility. Nor, did I hear how that spike in risk would or would not affect the public living next door or working at the businesses a couple of blocks away. CNN reported on March 4th “… patients and family members say they are left in the dark.” To me, officials basically communicated along the lines of: Just keep doing what you’re doing even if you live and work near the cluster-site.
A better approach would have included the following high performing systems “feedback and fix information” shown in green.
>> Initially, these containment steps went well.
>> These steps didn’t.
>> Here’s what we’re going to do to immediately improve containment and protect nearby residences and businesses.
>> Here’s what families can do if at-risk family members are in a cluster-site.
>> Here’s what care centers/hospitals in the state need to do if they suspect or have a spike in their facility.
This additional, honest and timely information would have better quelled local concerns/anxiety, would have increased confidence in fed-state-city containment officials, and would have quickly transferred learning to other front-line families and facilities. People would have felt better that help and corrections are on the way or have arrived.

Establishing the Kent city quarantine hotel
What went well. Seattle, Kent, and Kirkland cities are in King County. During March 4 and 5, King County announced it was establishing several quarantine centers distributed around their jurisdiction. This course of action has merit and appeared responsive to the rising number of citizens exposed to infected people. The Kent solution was creative. County officials quickly bought a motel that was up for sale. It was selected because individual rooms did NOT open into a common hallway and each room had individual HVAC so NO potentially-contaminated air circulated from room to room.
Plus, I believe the individuals assigned the task were busting their butts to get the sites up and running in days to better protect the public. Many people agreed with the need for Q-sites, while recognizing that the risk level was going to rise for people and businesses that would be close to the sites within the cities receiving the quarantine centers.
Three things did not go well.
#1 A pre-planned communication effort did not immediately emerge with the contractual and physical work to bring the Kent facility on-line. The mayor of Kent was not notified of the county’s plan to position a Q-site within her jurisdiction before county people showed up. She had to call the county. Neighboring businesses did not hear about the site until county personnel arrived at the hotel. Even the workers were not informed what would happen to their jobs. Most troubling was the county plan to allow quarantine folks to come and go at will. Upon hearing that, locals felt this was a dangerous plan that would guarantee spreading the virus to them. Compounding that belief was the mayor could not get the county to modify their plan and actually restrict people inside the Q-site. for 14-days. Thus, the City of Kent sued the county to stop the plan. That’s how poorly they judged the plan, the communications, and the cooperation they received from the county.
#2 At the beginning of the coronavirus outbreak Seattle-area elected officials appeared reluctant to forcibly constrain the movement of citizens via 14-day quarantines. Taking quick action that disrupts peoples’ lives was clearly a new behavior for state, county, and city officials. Unfortunately, it’s a once in a lifetime pandemic that requires new behavior. Yes, elected officials will be berated and disliked for constraining-actions that they must take to protect a broader group of people. Yes, the personal lives of many people and the finances of local businesses will be affected very quickly.
#3 Don’t name a quarantine-site a quarantine-site when it isn’t. Or restrict all quarantined people to stay on-site, within a fenced area, with delivered food and medical observation.
A better solution: When a containment action raises the risk level in a community, that risk will raise valid concerns within the locals and must be proactively and publicly addressed — not ignored. The final result may still be distasteful, but the public and their elected officials will not feel blindsided, used, and that their families and businesses are not important. Better cooperation will occur with better communication about restrictions when restrictions are needed and going to be imposed.

Preparing not panicking as the pandemic emerged
What went well. Health and Human Services Secretary Alex Azar, should be applauded for his ability to present a calm, determined, prepared, and informed demeaner when speaking to the public about preparing for the pandemic and about federal containment actions. His presentations before the first outbreak-cluster were good examples for other containment officials.
The good news is that millions of people from coast to coast are following his advice and the advice on CDC and state websites to prepare for a pandemic. This is easy for the millions who have previously prepared for natural disasters. For example, In California the public is encouraged to prepare for earthquakes and forest fires. Stocking up so a family of four can survive without electricity for 3 to 7 days is encouraged. Similarly, along the south-east coast of the United States, people prepare for hurricanes, as do people in tornado alley, stretching from Oklahoma to Ohio.
Conflicting Communications that did not work well. Officials below Secretary Azar, as well as doctors on media outlets repeatedly kept saying don’t panic and implied buying up limited items is panic behavior. The public has the right to know when does appropriate and encouraged preparation become panic? I can’t find on the CDC or state websites any explanation of what panic behavior looks like. CDC does say panic is a state of anxiety.
The communication problem is telling people to “prepare” then saying “don’t panic” when the bad behavior isn’t described. For example, if CDC feels panic behavior is hoarding or trampling others at Home Depot to buy the last few rolls of paper towels — then say so. Clarity is needed since one official’s panic is another person’s preparation.
For several reasons, it is not unreasonable and it is not panicking, to buy surgical, N95, and N99 masks at local stores to better fight off a coronavirus infection. For example, mothers or fathers are not panicking lunatics when they begin stocking the family pantry with extra food, medical, and cleaning items for a possible self-imposed or forced 14-day quarantine.
Their proactive efforts should be applauded. Unless they run over their neighbor with the car to get a package of sanitary-wipes, knock down a person to get into the pharmacy, or yank a case of soup out of another buyer’s arms.
Preparation also includes home-caregivers handling special needs at home where they are forced into close-proximity with a possible sick person. That is what they are supposed to do when handling people with pre-existing respiratory ailments or compromised immune systems. So, they should buy masks and that is not panic behavior.
The blanket advice for the remainder of the public to not buy masks unless they are sick, conflicts with the guidance to wear masks to protect others when you become sick. Being compliant requires each family to buy at least one package of masks. So, when are they supposed to buy the masks? To the man and woman on the street that means buy now and put the masks on the shelf in case someone in the family comes down sick later.
Advice about surgical masks, as if, the advice applies to N95 and N99 masks, or advice which is just not logical has caused many people to ignore CDC and state official about not buying masks. For example, here’s the advice issued while I was driving into Seattle just before the virus-crap hit the fan in Kirkland. A public health officer from the Seattle area said:
“Masks really don’t block the particles. . . “Air can come around the side of them and you can inhale the droplets if someone close to you is coughing or sneezing.”

>> We won’t inhale the droplets when we are NOT wearing a face mask near a sneezing person?
>> Wearing a mask will NOT reduce the amount of infected moisture inhaled?
>> We get sick if we breathe in the coronavirus, so trying to filter out infected air with any mask is bad?
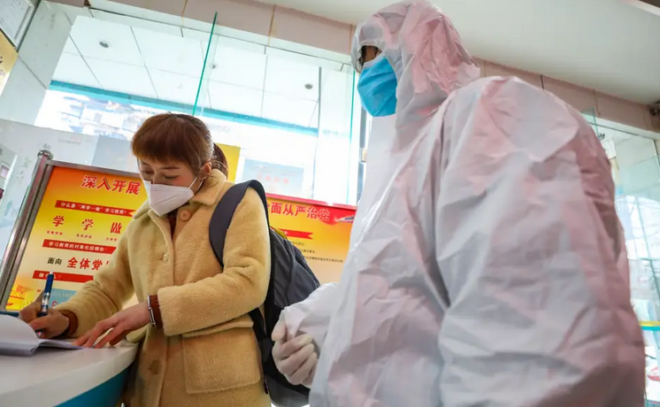
Advice that masks don’t work also conflicts with what many people see at coronavirus scenes. For example, millions of Americans have watched many quick-reaction and medical caregivers, in other countries and at the Life Care Center of Kirkland, wearing masks. Is it because the firemen, EMT, and emergency room personnel expect the people they will encounter are often sneezing or coughing? Possibly. Or is it also because masks, especially N95 and N99 masks, do increase a person’s protection along with other means of prevention, even when people are not sneezing?
Advice that masks don’t work conflicts with the real-world condition that, crap happens. For example, there I was in Kent, Washington because a family member was in ICU after a complication during a surgery. Of course, I drove to the Seattle area to be with the family.
But being well informed about the coronavirus, I’m keeping my social distance, not riding the elevator in my motel, washing my hands often, using sanitary wipes to clean my truck, as well as doorknobs into my room, and placing a do not disturb sign so cleaning people stay out of my room. Plus, I’ve had this year’s flu inoculation. I’ve been doing everything right in an area where the health officials say 200 to 300 people may be infected but are unknown in the community .So, no need to wear my N95 mask, even though I brought protection supplies for all my nieces and their loved ones because those items were sold out locally.
Then, the day before I leave town I’m walking down the hallway to get to my room. Just before I reach the alcove where the elevators are, I hear a huge cough. And I’m blasted by a woman who didn’t cough into her elbow because she didn’t know anyone was coming down the hallway. Immediately I wish I was wearing my mask.

Four days later and I’m at home. Despite always telling people I’m “strong like bull” I’m in a susceptible group. I’m over 65. So, I’m self-quarantining myself. And guess what? I woke up today with a scratchy throat, have coughed a few times, plus a headache. Hopefully, I’m just feeling poorly from all the hours I spent driving 2,000-miles to avoid planes routinely flying into and out of SeaTac airport. Only 10 days to go.
The last conflicting communication is advising people they don’t need to buy masks because federal officials say the country is critically short of prevention items for hospital and quick reaction care givers. Unfortunately, the communications issued before or since the Kirkland Life Care Center outbreak have never addressed federal and state actions to increase quantities of caregiver protection items, except test-kits.
Thus, it is not panic for a person to feel that federal and state health officials should have been contracting for millions of masks once the coronavirus started arriving in the U.S. in January. So, now that the virus is infecting and killing locals, folks are going to finish preparing by buying what is on the shelf for their families.
Eliminating conflicting communications
If federal and state contracts have been signed, I encourage Secretary Azar and officials to share that information with the public. Plus, they could request that the public only buy 1 package of masks per household and have restraint on purchasing other items during the coming 30 days.
Had the containment team shared the contracting-status then their request for restraint by the public might have slowed some of the buying. Even if it didn’t, the less confusing and more direct messaging would increase the trust for advice coming from the multi-agency containment team trying to squash the pandemic.

Conclusion: Well-meaning advice for low-risk pandemic-areas, needs to be accompanied with well-meaning advice about what to do when the virus-crap hits the fan.
It is human nature to buy available products that can help protect one’s family from a forest fire, hurricane, tornado, or pandemic. The federal government has the means to contract for large amounts of critical materials for distribution as it sees fit. Encouraging public-buyers to delay purchases is unlikely to prevent local stock of critical material, like face masks, from being unavailable to the government.
Meanwhile, millions of citizens will decide when to self-mask but could be influenced by the government’s containment experts on when to use self-masking with other self-protection techniques during high-risk pandemic conditions.
Recommended standard operating procedure
Before this pandemic ends its course through the USA, other cities will see cluster-spikes within their jurisdictions. Hopefully, not as bad or worse than what Kirkland is facing. Therefore, containment officials from the Vice-President to local health officials should conduct a daily status meeting that asks-and-answers the following questions for their jurisdiction. Then, periodically communicate the truth to the public.
>> What are the containment and outbreak trends in the last 7-day period?
>> What is the change in the infected-recovered-died statistics in the last 24-hours
>> What containment actions have gone well in the last 24-hours?
>> What’s not gone well?
>> What fixes have we implemented or are needed?
Recommended questions to be answered by federal and state task forces
>> When does appropriate and encouraged preparation become panic?
>> Are people living or working next to a high-risk facility at higher risk of catching the new coronavirus?
>> Are people safer from becoming infected by self-masking in their residence, or business next to a highly-infected site?
>> What is the criterion for closing a local business near a highly-infected site?
>> Several cruise ships have had coronavirus clusters. Similar to Legionnaires Disease, can the new coronavirus infect people after blowing through the ventilation system on cruise ships?
>> Why is it okay to self-quarantine but not self-mask?
>> Under what risk-conditions is it appropriate to self-mask?
>> When and how many millions of protection-gear has the federal government contracted for, before and since the Kirkland Washington Life Care Center outbreak?
Encouragement for containment teams
In the 4th thriller in my series, The Destiny Relic, I write about using the MERS coronavirus to achieve a security goal in the Middle East. Associated with that incident is a verse from the bible, which may provide a useful perspective for containment teams and families on the front line of the coronavirus-pandemic. “I have set before you life and death, blessing and curse. Therefore, choose life, that you and your seed may live.”
From: Author Ed Mitchell
Click to contact me direct
(Also on GoodReads)
Please Share This with your social media friends.
Share This On – Facebook
Tweet This On – Twitter OR Messenger This On – Facebook Messenger
Autographed award-winning thrillers are available at my website
Encourage your social media friends to sign up for one or more of my blogs
All Titles are available as an autographed physical copy (spend $25 or more and shipping is free) or in Kindle format on Amazon .